Prevention-First Healthcare Just Got $150M in Validation. Here’s What It Means for Your Practice.
Effie Arditi
Co-Founder & CEO
Share:

Why One Insurance Company’s Funding Round Matters More Than Any Longevity Research
Last month, Curative closed a $150 million Series B round. For practitioners running longevity and functional medicine practices, this funding announcement deserves more attention than any NAD+ study you’ll see this year.
The reason is simple: Curative operates as a health insurance company, not a research institute or supplement brand. They’re wagering that preventive healthcare delivers superior financial performance compared to conventional treatment-based models.
Their approach removes every financial barrier for members who complete preventive annual assessments. Zero copays, zero deductibles, zero coinsurance.
The numbers back their strategy: primary care visits increased 20%, hospital admissions dropped 30%, and prescription costs fell up to 40% in year one.
An insurance company just secured nine-figure funding to demonstrate that stopping disease beats treating it – not just for patients, but for profit margins.
Prevention transitioned from theory to investment thesis. This shift opens major doors for practices ready to deliver at scale while exposing serious gaps for those unprepared.
The Economics Driving This Transformation
American employers now allocate over $1 trillion toward employee health benefits annually. This spending makes them the nation’s dominant healthcare purchasers.
Yet they face a contradiction: premiums increase 5-7% yearly while workforce health deteriorates. Traditional approaches fail both their financial objectives and their people.
They’re seeking alternatives. Programs that cut long-term expenses, boost workforce productivity, and deliver quantifiable returns.
Insurance companies responded by designing prevention-centered offerings. Their core question shifted from “how do we process claims efficiently?” to “how do we prevent claims from happening?”
This transformation creates genuine demand for your clinical model. Corporate buyers want preventive services. Insurers are structuring payment mechanisms to support them. Market opportunity exists. Opportunity, however, does not equal access. Participation requires operational readiness.
Three Converging Trends Behind the Opportunity
Three distinct market shifts aligned over the past 18 months to create this moment.
1. Financial Incentives Rewired Around Health Maintenance
Curative represents one data point in a broader pattern. Value-based care contracts expanded 25% throughout 2024. Direct primary care enrollment jumped 30% year-over-year. Accountable care organizations now serve more than 50 million people nationwide.
These models share a fundamental trait: they tie financial performance to maintaining wellness rather than billing for illness.
They require clinical partners capable of delivering preventive services at meaningful volume. Not routine check-ups with standard blood panels. Genuine prevention: detailed biomarker profiling, targeted lifestyle modifications, ongoing monitoring, early dysfunction detection.
This matches your clinical practice and the payment infrastructure being constructed needs your methodology.
2. Longevity Interventions Achieved Clinical Application
Therapies addressing cellular aging, metabolic dysfunction, mitochondrial decline, and epigenetic modifications progressed from university labs to patient trials during 2024.
Organizations commercializing these treatments need clinical distribution networks. They need practitioners fluent in systemic medicine, personalized interventions, and rigorous outcome measurement. They need practices equipped with data capabilities to support trials and document effectiveness.
Your practice already operates this way. The barrier is whether you possess systems enabling scaled participation.
3. Operational Gaps Became the Bottleneck
Payers want preventive services. Scientific advances enable better treatments. Patients demand personalized, proactive healthcare.
Yet most preventive practices operate on disconnected infrastructure:
- Health information fragmented across electronic records, laboratory systems, wearable platforms, and manual documentation
- No consolidated perspective on patient health evolution
- Manual processes for tracking compliance and results
- Weak capability to validate return on investment for corporate or insurance buyers
- Absence of standardized population health reporting
You provide exceptional individual patient care. But can you validate outcomes across 500 patients? Can you produce the documentation payers require for payment authorization? Can you expand operations without multiplying administrative burden?
This bottleneck explains why most preventive practices cannot access the prevention economy despite strong market demand.
Clinical Governance Infrastructure vs. Administrative Tools
Solutions require more than improved software. They demand a fundamentally different operational approach.
Unified Health Data Architecture
Each patient produces information from diverse channels: clinical encounters, laboratory testing, genetic analysis, continuous monitoring devices, self-reported metrics. Most practices store this information in isolated systems.
Unified architecture consolidates these streams. Not merely centralizing storage, but synthesizing information into coherent longitudinal records that expose trends, reveal patterns, and support prediction.
This foundation proves essential. Without it, you deliver reactive interventions disguised as preventive care.
Adaptive Protocol Engines
Generic programs produce mediocre results. Effective prevention demands customization based on unique biomarkers, genetic makeup, behavioral patterns, and individual objectives.
Yet customization at volume requires intelligent automation. You need systems that modify protocols based on response data, monitor compliance, detect inadequate responses, and support clinical decisions without creating information overload.
The objective isn’t eliminating physician judgment. It’s extending it by managing complexity beyond human processing capacity.
Population Health Analytics
This represents the failure point for most preventive practices operationally. Your interventions produce results. Individual patients improve. But can you validate this pattern systematically?
Corporate buyers and insurance companies require specific answers:
- What proportion of your patient population shows improved metabolic function?
- How many patients avoid developing chronic conditions?
- What magnitude of biological age reduction do you achieve on average?
- Which protocols generate optimal results for specific patient profiles?
Without evidence-based responses, you cannot secure performance-based contracts. You cannot validate financial returns to employers. You cannot build the research foundation that establishes preventive medicine credibility.
Physician Control Framework
This distinction separates infrastructure from simple automation. Clinical governance ensures physicians maintain decision authority.
Artificial intelligence recognizes patterns. Algorithms highlight significant deviations. Systems recommend interventions. But clinical confirmation, protocol authorization, and treatment choices remain under physician direction.
This matters beyond quality assurance. It establishes trust. Corporate buyers, insurance companies, and patients need assurance that preventive services maintain rigor, evidence foundations, and medical supervision. Opaque algorithms undermine confidence. Physician-directed platforms build it.
What Growth Looks Like Without Proper Systems
Consider the practical implications for a preventive medicine practice attempting expansion.
Actual Example: Growing a Functional Medicine Practice
Your functional medicine practice succeeds. You conduct 20-30 patient visits each week. You order detailed laboratory panels, monitor biomarker changes over time, design individualized protocols, and document strong patient outcomes.
A regional employer approaches you. They want to provide your services to 500 employees as a preventive health benefit. They propose a fixed monthly fee per employee. They expect quarterly performance reports documenting participation rates, health metric improvements, and financial value generated.
Can your practice accept this contract?
Using your existing operational setup?
- How do you monitor 500 individual patient progressions across dozens of biomarkers?
- How do you generate hundreds of customized protocols?
- How do you track compliance and identify patients requiring intervention?
- How do you compile outcome information for quarterly reporting?
- How do you absorb the administrative workload without massive staff expansion?
Without appropriate infrastructure, this growth opportunity transforms into an operational nightmare. You either decline the contract (forgoing revenue and impact) or accept it and suffocate under manual workload that eliminates time for patient care.
This operational bottleneck blocks practice growth despite market demand.
Our Solution at Longevitix
We developed Longevitix after recognizing this gap from clinical practice. Preventive medicine produces results. Scientific foundations are robust. Patient improvements are documented. But operational frameworks to deliver these results at volume were absent.
We built the missing infrastructure:
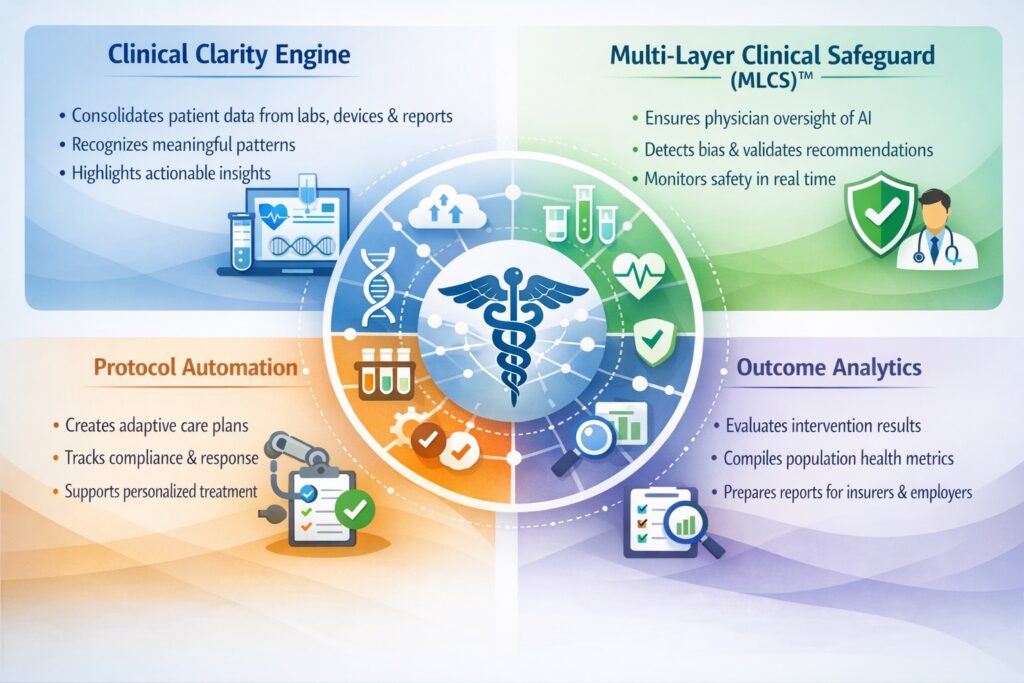
Clinical Clarity Engine: Consolidates patient information from laboratories, monitoring devices, genetic testing, and patient reporting into longitudinal health trajectories. Recognizes meaningful patterns across information streams. Highlights actionable insights while eliminating irrelevant data.
Multi-Layer Clinical Safeguard (MLCS)™: Maintains physician authority over AI-generated recommendations. Includes clinical validation requirements, algorithmic bias detection, real-time safety protocols, and ongoing monitoring. Technology enhances rather than supplants physician expertise.
Protocol Automation: Generates individualized prevention strategies that evolve based on patient response. Monitors compliance, identifies inadequate responses, supports clinical decision-making. Enables personalized medicine at scale without proportional workload growth.
Outcome Analytics: Compiles population-level health metrics. Evaluates intervention performance. Produces documentation for insurance companies, employers, and quality assessment. Transforms individual care into verifiable population results.
This transcends practice management applications. It provides operational infrastructure enabling preventive medicine practices to participate in the emerging prevention economy funded by companies like Curative.
The Window for First-Mover Advantage Is Closing
The prevention economy advances regardless of current practitioner participation.
Without operational systems enabling scaled delivery, other players will capture this market. Large hospital systems will establish “preventive care divisions.” Technology companies will launch consumer-facing platforms. Insurance companies will contract with any provider demonstrating outcome measurement and population health management capabilities.
Your clinical knowledge holds value. Your patient relationships matter. Your documented results are genuine. But specialized knowledge without supporting infrastructure cannot scale. In markets where insurance companies invest hundreds of millions in prevention-focused models, scalability determines market access.
You hold strategic advantage. You’ve practiced this approach for years while mainstream medicine dismissed it. You understand causal interventions, interconnected systems thinking, and customized protocols. You know biomarker interpretation and trajectory analysis.
What you need is operational infrastructure enabling delivery at market-demanded scale.
Three Essential Self-Assessment Questions
Can you validate outcomes at population scale?
Individual success stories create powerful narratives. But corporate and insurance buyers require aggregated evidence. Without demonstrating that specific percentages of patients achieve defined improvements within specified timeframes, you cannot compete for performance-based contracts.
Can you expand patient volume tenfold without proportional staff growth?
Growth demands systematic infrastructure. If patient volume doubles requiring staff doubles, your model lacks scalability. Seek infrastructure automating data consolidation, protocol development, compliance monitoring, and outcome documentation.
Does your platform meet regulatory and payer standards now?
Corporate and insurance contracts impose compliance obligations, data protection requirements, and outcome validation protocols. Your infrastructure must satisfy these standards immediately, not after securing your first major contract.
Market Timing Advantages Don’t Guarantee Market Winners
Preventive medicine practitioners have advocated the correct healthcare model for decades. You’ve addressed underlying causes while others symptom-managed. You’ve tracked patient progressions while others examined isolated moments. You’ve prevented disease development while the system waited for diagnosis.
Market validation finally arrived, but market validation doesn’t automatically benefit early advocates. The prevention economy will develop regardless. What remains uncertain is who captures the value.
Will market benefits flow to practitioners who pioneered preventive approaches but lack scaling infrastructure? Or to well-funded entrants who understand operational systems but lack clinical depth? Historical patterns suggest the latter prevails unless the former builds necessary infrastructure rapidly.
Data-driven markets don’t reward paper-based operations. Performance-based contracts require performance measurement systems. Personalized medicine at scale demands automated personalization. Clinical innovation emerged from your practices. Operational innovation must follow.
Frequently Asked Questions
Why are prevention-first models becoming financially attractive now?
Corporate healthcare spending exceeds $1 trillion annually while employee health declines. Prevention-focused approaches like Curative’s demonstrate 30% hospitalization reductions and 40% prescription cost decreases in year one, proving prevention generates superior financial returns compared to treatment-based care.
How do performance-based insurance contracts function for preventive practices?
Performance-based agreements link payment to documented patient improvements rather than service volume. Practices must validate measurable outcomes—such as biomarker improvements or disease prevention rates—across entire patient populations to qualify for these payment structures.
What operational capabilities do practices need for prevention economy participation?
Practices require consolidated patient data platforms, automated protocol customization, population-level outcome measurement, and physician-supervised AI safety frameworks. Without these capabilities, scaling preventive care becomes operationally unmanageable despite existing demand.
Why do standard practice management systems fall short?
Practice management applications handle appointment scheduling and payment processing. Prevention economy participation demands longitudinal data synthesis, personalized protocol automation, population health analytics, and insurance-grade outcome documentation—capabilities absent from most practice management solutions.
How rapidly is the prevention economy expanding?
Performance-based care arrangements grew 25% during 2024. Direct primary care membership increased 30% annually. Accountable care organizations currently serve over 50 million Americans. Major investments like Curative’s $150M round signal accelerating market maturation.
What risks face practices that delay adaptation?
Practices lacking scaled delivery infrastructure will lose market access as corporate buyers and insurance companies contract with providers demonstrating outcome measurement and population health management. Clinical expertise alone proves insufficient for securing performance-based contract participation.



