How to Operationalize Personalized Longevity Care in a Clinic
Effie Arditi
Co-Founder & CEO
Share:
What it means to operationalize personalized longevity care
A few months ago I was on a call with the founder of a longevity practice on the East Coast. She has a waiting list, a beautiful clinic, two excellent physicians, and a patient experience people post about. She also told me, fifteen minutes in, that she hadn’t slept properly in a year. The clinic was working. She was the one breaking under it.
That conversation is, more or less, the reason this article exists. To operationalize personalized longevity care in a clinic is to turn what a great physician can do for one patient into something a small team can do, consistently, for hundreds, without grinding the founder into dust along the way. It is not a marketing posture, and it is not a more expensive intake. It is a quiet decision about plumbing: data, workflows, protocols, and follow-up loops that hold up when the panel doubles.
I’m watching dozens of clinics try to grow – most of them are stuck in the same place and for the same reason.
Why the existing healthcare system was not built for personalized longevity care
The system we work inside was designed around acute episodes. Someone gets sick, the system reacts, the system bills. Personalized longevity care does the opposite. It tracks people who feel fine, looks for trajectory changes, and intervenes years before any acute event. The two models share almost no infrastructure.
Think about what a standard EHR actually is. It’s a charting and billing engine. It is not a longitudinal record. It was never meant to surface a fifteen-year drift in fasting insulin or correlate sleep architecture with HRV. A standard primary care panel of 1,500 to 2,500 patients per physician is a workable load if you’re managing episodes; it’s an impossibility if you’re managing trajectories. A 12-minute visit is enough to refill a statin and not enough to talk through ApoB, a CGM trend, and a strength training plan in the same conversation.
When a clinic chooses to deliver personalized longevity care inside infrastructure that was built for the opposite, every gap shows up somewhere. Usually it shows up first as the founder physician working until 11 p.m. on chart review, and eventually as the clinic quietly delivering a less personalized version of the care it set out to provide.
Five tests of an operationalized longevity clinic
When I look at the practices that scale well versus the ones that struggle, the difference shows up in a handful of small, observable things. A clinic is operationalized when:
A new patient can move from intake to assessment to plan to follow-up without anyone on the team improvising at each step. Two physicians in the same practice produce comparable plans for comparable patients. Data captured at visit one is still usable, comparable, and visible at visit twelve. Staff turnover doesn’t break the model. The panel can grow without growing physician hours at the same rate.
If you can hold those five lines, the rest is tuning. If you can’t, you have a great practice held together by a small number of heroic people. That works for a while. It doesn’t work forever, and the people holding it together know.
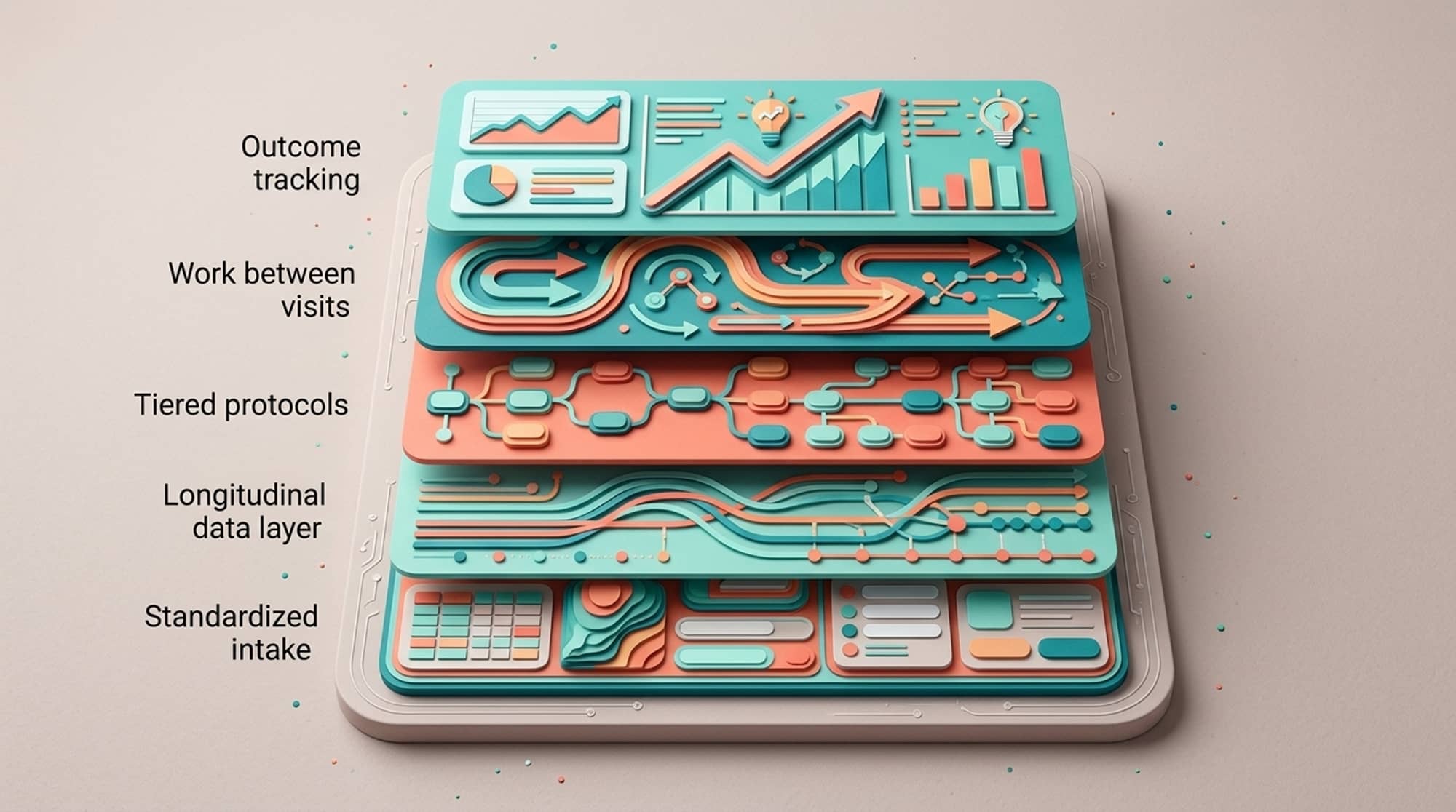
The five infrastructure layers every longevity clinic needs, in build order
The list isn’t that controversial. The order is. Most clinics get the list right and the order wrong, and that’s almost always the source of the year-two crisis.
Start with standardized intake. Same questions, same units, same fields, same place. It sounds boring because it is boring, and it’s the boring decision that makes everything downstream possible. If three patients can have their ApoB or VO₂ baseline recorded in three different formats, your data is broken on day one and nobody will notice for two years.
Then build the longitudinal data layer. This is the one most clinics underbuild, and it’s the one that breaks first. Labs from Quest at year one have to be comparable to LabCorp at year three. Wearable data has to flow continuously, not get reviewed in a quarterly batch. Imaging needs structured metadata, not just PDFs sitting in a folder. Family history and prior records need to be reconciled into one timeline, not stored as an inbox of uploads. A 2026 analytical framework for healthy longevity clinics makes the same point in clinical language: the data layer is the foundational component, not a feature. Most of the practices we work with figured that out the hard way, somewhere in their second year, when a patient asked a question they couldn’t answer because the data lived in five places.
Only then do tiered protocols make sense. Personalization doesn’t mean every patient gets a custom plan written from scratch. It means the standard plan is well-engineered, and the parts that vary are documented decisions rather than improvisation. The shape I see working is roughly: a universal tier (sleep, training, nutrition, basics), a risk-stratified tier (lipids, glycemic management, blood pressure, bone health), an individualized tier (hormones, GLP-1 candidacy, advanced surveillance), and a referral tier. The 2025 Longevity Medicine recap from Longevitydocs put it bluntly: the field scaled faster than its foundations. The practices that wrote down their protocols are the ones not strained right now.
Then design the work between visits. This is where most clinics underestimate the load. CGM reviews, wearable trend flags, lab follow-ups, patient messages, plan adjustments. If nobody has decided who does what when, the physician absorbs all of it. That is the year-two burnout pattern, and it is almost never solved by the physician working harder. It is solved by structure: a defined cadence, clear ownership, automated triggers for the things that don’t need a physician, and physician time reserved for the things that do.
Finally, outcome tracking. If you can’t describe what your clinic produces, you can’t improve it and you can’t make the case for it to anyone outside the room. Process metrics, biomarker trajectories at the panel level, patient-reported outcomes, hard outcomes over time. This is also the language you will need when employers and payers come to the table. They are starting to, as the longevity clinic infrastructure market expands and membership models grow as a share of the service economy.
How longevity clinics break as the panel grows
Most of the founders I talk to recognize the pattern almost immediately, because they have lived in some part of it.
At fifty to a hundred patients, the founder is doing everything. Protocols live in their head. Quality is excellent because the founder is excellent and the volume is small. The model feels like it works, and in a sense it does.
Around two hundred to three hundred patients, the same physician starts running out of hours. Wearable data piles up. Labs get ordered but reviewed in isolation, not in trajectory. The first patients to fall through the cracks are the ones who feel fine, because nothing forces their case to surface. This is the moment most founders first realize the operational layer they didn’t build is now actively missing.
Past five hundred patients, without that layer, the choices narrow. The clinic caps growth, hires more physicians at proportional cost, or quietly delivers a less personalized version of the care it promised. We’ve watched all three play out, sometimes in the same practice in different quarters. None of those outcomes are clinical failures. They are infrastructure failures that show up clinically. The clinics that get past five hundred patients per panel without losing quality almost always built the operational layer earlier than felt reasonable at the time.
Staffing model for a 500-patient personalized longevity panel
The composition I see consistently working at this size: one physician trained in longevity, preventive, or internal medicine; one NP or PA; one health coach focused on nutrition, behavior change, and exercise; about half an RN for care coordination, lab follow-up, and message triage; and a part-time operations or data role, often shared across panels.
That last one is the role most clinics skip. It is also the role that most directly determines whether the clinic is genuinely operationalized or simply very busy. A great clinical team without an operational counterpart will recreate, by hand, the work that good infrastructure should be doing in the background. They’ll do it well for a while, and then they’ll get tired.
Where personalized longevity care is headed in 2026
The WEF’s 2026 take on preventive medicine and most credible market analyses converge on the same point: preventive longevity care is moving from boutique to infrastructure. The clinics that win the next five years won’t be the ones with the most expensive intake or the most premium real estate. They will be the ones that can deliver consistent personalized care at a panel size where the economics actually work.
That requires building the parts patients never see. Data plumbing. Protocol libraries. Between-visit workflows. Outcome dashboards. The clinical work is the visible craft. The operational layer is what makes it repeatable, year after year, across hundreds of people. (We’ve written more about this pattern in 7 Critical Challenges Preventive Medicine Clinics Face and in Everyone Has AI Now. So Why Is Healthcare Still Broken? for anyone who wants to keep pulling on the thread.)
Key takeaways on operationalizing personalized longevity care
Personalized longevity care does not scale on physician effort. It scales on infrastructure. The founders I respect most are the ones who decided, well before they had to, to build the operational layer underneath the clinical work: standardized intake, longitudinal data, tiered protocols, between-visit workflows, outcome tracking. They were less impressive in year one than the founders who poured everything into the patient experience. They are the ones still standing without strain in year three.
The patient experience and the operational layer aren’t a tradeoff. The operational layer is what protects the patient experience as the panel grows, and what protects the founder from being the single point of failure for the model.
FAQs
What does it mean to operationalize personalized longevity care in a clinic?
Operationalizing personalized longevity care means turning individualized assessment, planning, and follow-up into a repeatable workflow that a small team can run consistently for hundreds of patients. It requires standardized intake, longitudinal data infrastructure, tiered protocols, between-visit workflows, and outcome tracking. A clinic is operationalized when two physicians produce comparable plans for comparable patients without improvising at each step.
How many patients can one physician realistically manage in a longevity clinic?
A typical operationalized longevity panel runs 200-500 patients per physician, compared to 1,500-2,500 in traditional primary care and 300-600 in concierge or DPC. The exact number depends on visit length, the supporting team, and how much between-visit work is automated. Without an operational backbone, quality typically degrades past 300 patients per physician.
What infrastructure does a personalized longevity clinic need before it scales?
Before scaling, a clinic needs a unified longitudinal record ingesting labs, wearables, imaging, family history, and prior records into a single normalized timeline. It also needs documented tiered protocols, a defined visit cadence, between-visit workflows, and outcome tracking at the patient and panel level. Most clinics that fail in year two underbuilt this layer in year one.
How is operationalized longevity care different from concierge medicine?
Concierge medicine reduces panel size and increases visit time, but does not by itself produce personalized longevity care. Operationalized longevity care adds longitudinal data infrastructure, tiered documented protocols, integrated wearable data, and outcome tracking on top of the concierge time model. Time alone is necessary but not sufficient.
Why do longevity clinics often break around 200-300 patients?
At 200-300 patients per physician, the clinic typically outgrows the founder’s ability to hold the model in their head. Without documented protocols, longitudinal data infrastructure, and structured between-visit workflows, the physician absorbs work that should be handled elsewhere. The clinic either caps growth, adds physicians at proportional cost, or shifts toward a less personalized model.
What outcomes should a longevity clinic track to show that its care works?
Track process metrics (screening and protocol adherence), biomarker trajectories at the panel level, patient-reported outcomes, and hard outcomes over time including incident cardiovascular events, new cancer diagnoses, fractures, and hospitalizations. Outcome tracking is also what makes credible payer and employer conversations possible as the membership-based longevity care market expands.
Why is longitudinal data infrastructure the most important investment for a longevity clinic?
Personalized longevity care depends on detecting trajectory changes (out-of-pattern values) rather than single out-of-range results. That requires unified data across labs, wearables, imaging, and family history over time, normalized so values from different sources and dates are comparable. Clinics that skip this layer end up making personalized recommendations from a partial picture.
What roles does a 500-patient longevity clinic typically need?
A working composition is one physician, one NP or PA, one health coach, half an RN for care coordination and message triage, and a part-time operations or data role often shared across panels. The operations and data role is the one most clinics skip and the one that most directly determines whether the clinic is operationalized or just busy.



