The Single Aging Clock Is Over: How Foundation Models Are Changing Biological Age Measurement

Gaby Hayon
Co-Founder and CTO
Share:

For most of the last decade, a patient’s biological age arrived as a single number. You drew blood, sent it to a lab running an epigenetic clock, and weeks later a value came back. Forty-seven. Fifty-two. The number felt scientific because it was precise. Precision and accuracy are not the same thing, and the distance between them is exactly why many used these tools cautiously in the clinic. A confident-looking number built on one narrow slice of biology can still be wrong in ways that matter for a real patient.
That single-number era is now ending, and the reason is worth understanding for any physician building a preventive medicine practice.
Why a single epigenetic clock was always a compression of biology
Aging shows up in many places at once. It appears in methylation patterns, in circulating proteins, in gene expression, and in the slow drift of dozens of clinical markers over years. A clock built to output one value from one data type was always a compression of something far richer. A model that reads only one of those streams is listening to a single instrument and trying to describe the whole orchestra. That is true even for the well-validated clocks clinicians know, such as GrimAge, PhenoAge, and DunedinPACE. Each is excellent at the narrow job it was trained for, and each sees only part of the picture.
What foundation models for aging actually do
This is where the field is heading next, and the shift is captured well by a paper published this spring titled “The End of Aging Clocks: Training Foundation Models to Reason in Aging and Longevity”. The argument is straightforward: a narrow algorithm trained to predict one value is fundamentally limited, so the better path is a large model trained across many data types at once, then asked to reason about what it sees.
From one data type to multimodal reasoning
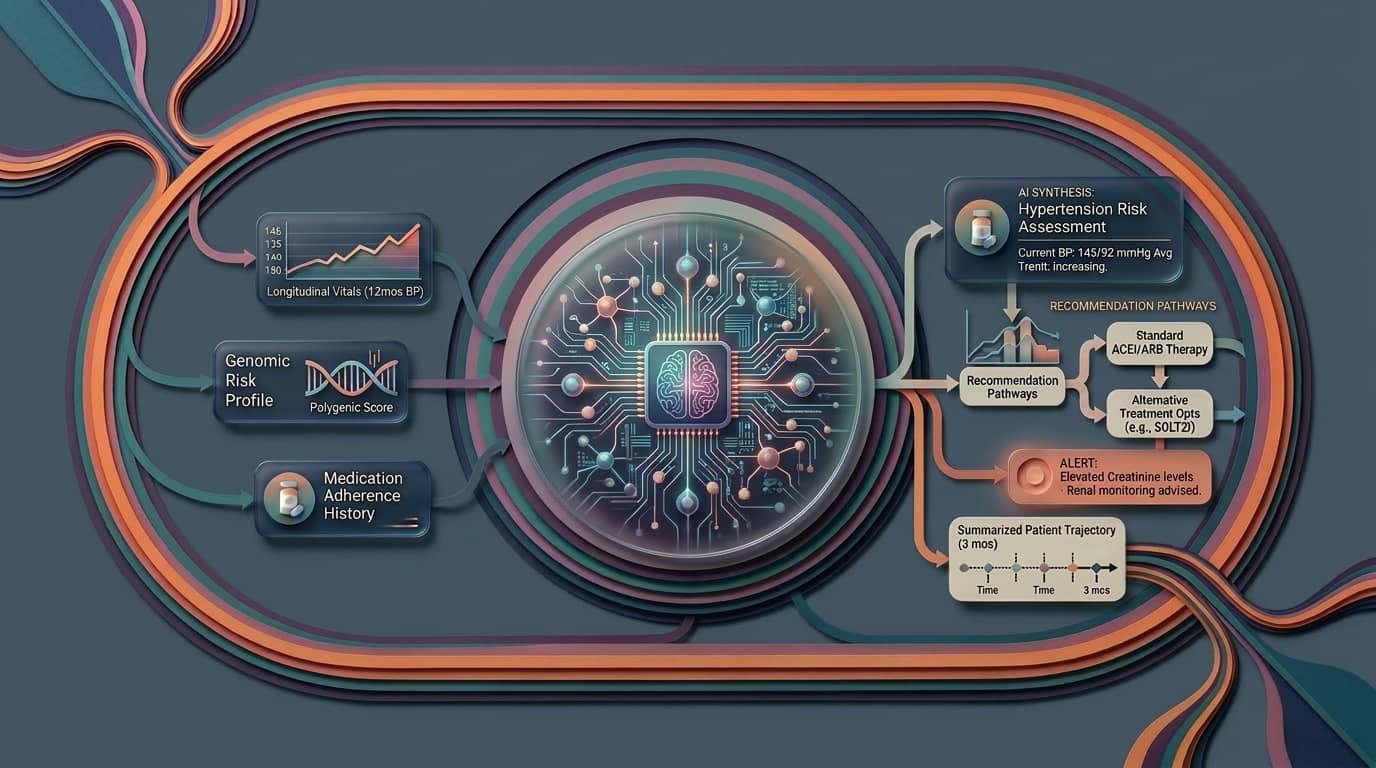
A foundation model does not simply output a verdict. It integrates genomic, proteomic, imaging, clinical, and longitudinal signals into one coherent read, and it can be interrogated about that read. The frame moves from measurement to reasoning. Instead of asking “what number does this assay produce,” the clinician can begin to ask “what in this patient’s biology is driving the result, and how confident is the model.”
Early results: Longevity-LLM and the first longevity foundation model
The early evidence is encouraging. Longevity-LLM, an initial version released this spring, was fine-tuned on DNA methylation, proteomics, clinical biomarkers, and RNA expression together. It predicted epigenetic age with a mean error of roughly 4.3 years, better than the original Horvath multi-tissue clock that helped define the field. The accuracy is not the real headline. The headline is that one model held four kinds of biology in view at the same time. The industry is moving the same way with serious capital behind it. In May, Insilico Medicine and Human Life Foundation Models announced a collaboration to build the first large-scale foundation model dedicated to human longevity science, trained on genomic, proteomic, imaging, clinical, and longitudinal health data. Insilico had already formed a dedicated longevity board in April to steer exactly this kind of work.
What reasoning models change at the exam table
A single clock hands you a verdict. A reasoning model opens a conversation. When a model integrates many signals, it can begin to surface which signals are driving an accelerated read, whether a patient’s proteomic profile and methylation profile agree, and where they part ways. That is the kind of output a physician can actually act on. A lone number tells you something is off somewhere. A model that reasons across biology starts to tell you where to look first.
A point I keep returning to with colleagues: these are probabilistic systems, not oracles. A model that reasons fluently can also reason confidently when the underlying data is thin or noisy. That is not a flaw to hide, it is a property to manage. The output is a well-informed estimate that a clinician weighs against the rest of the picture, not a decree that replaces judgment. Used that way, the probabilistic nature becomes a strength, because the model can express uncertainty and point to what would resolve it.
The catch: model output is only as good as the data underneath
All of which leads to the unglamorous truth underneath the breakthrough. The quality of what comes out depends entirely on the quality and completeness of what goes in. A patient with three lab panels scattered across two years and a wearable that synced intermittently does not give even a sophisticated model much to reason with. The most advanced longevity model in the world reads a fragmented record and produces a fragmented answer.
What this means for longevity clinics
This is the part our team thinks about constantly. These models are only as good as the longitudinal record they read from, and most clinics are still assembling that record by hand. Labs live in one system, wearable data in another, the clinical history in a third. Before any reasoning model can do something useful for a specific patient, someone has to unify that patient’s data into a clean, continuous, structured picture. The model is the engine. The unified record is the fuel. We built our platform around that second half precisely because the first half is finally arriving, and clinics with a real data foundation will be ready to put these tools to work the moment they mature.
The shift from clocks to reasoning models is good news for preventive medicine. We are moving from a single annual verdict toward a living, multimodal read of a patient’s biology that a physician can interrogate and explain. The number was never the point. Understanding what drives it always was.
Frequently asked questions
What is a foundation model for aging?
A foundation model for aging is a large artificial intelligence model trained across many types of biological data at once, including methylation, proteomics, gene expression, imaging, and clinical markers. Rather than producing a single biological age from one assay, it reasons across these inputs to estimate aging and to surface what is driving the result.
Are AI aging clocks accurate enough for clinical use?
Accuracy is improving quickly. Early multimodal models such as Longevity-LLM have already outperformed first-generation epigenetic clocks on age prediction. For clinical use, the more important point is that these are probabilistic estimates meant to support a physician’s judgment, not to replace it, and their reliability depends heavily on the completeness of the patient data behind them.
Do foundation models replace epigenetic clocks like GrimAge or DunedinPACE?
Not exactly. Established clocks remain useful and well-validated for the specific outcomes they were built around. Foundation models aim to integrate the signals those clocks capture, alongside many others, into a single reasoning system. Think of it as a broader layer that can incorporate existing clocks rather than discard them.
What does a clinic need to use these tools effectively?
The essential prerequisite is unified, longitudinal patient data. Labs, wearables, imaging, and clinical history need to live in one structured record so the model has something coherent to reason from. Clinics that solve data unification first will get far more value from longevity AI than those running the most advanced model on fragmented inputs.